Systemic Vulnerabilities of India’s Healthcare Infrastructure in Addressing Waterborne Infections and Heat-Related Morbidities
Introduction
Climate change as a public health crisis reflects the interaction between environmental stressors and human health systems. According to global health assessments, nearly 3.6 billion people already live in highly climate-vulnerable settings, with India emerging as one of the most exposed regions due to its tropical geography, high population density, and uneven infrastructure.
Rising temperatures, erratic rainfall, and extreme weather events are intensifying waterborne infections such as cholera, typhoid, leptospirosis alongside heat-related morbidities like heat stroke, cardiovascular stress, and renal dysfunction.
This dual burden exposes deep systemic vulnerabilities in India’s healthcare architecture, particularly in terms of preparedness, accessibility, and adaptive capacity.
Body
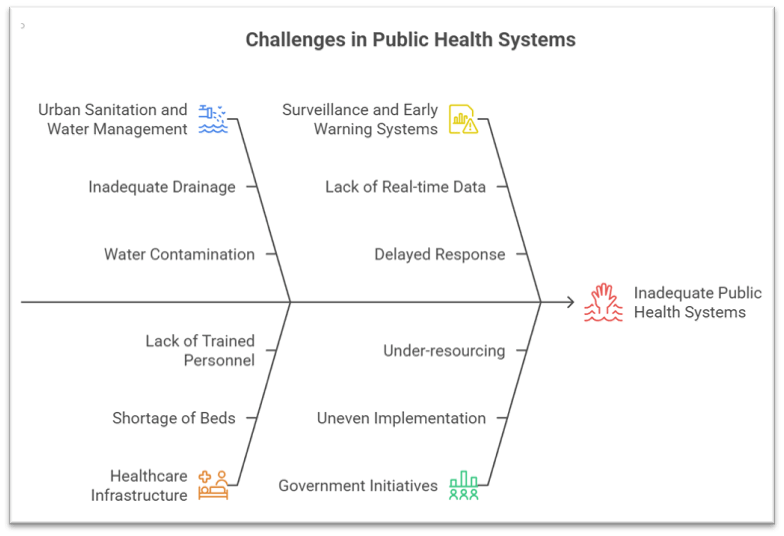
1. Structural and Infrastructure Deficits in Public Health Systems
Inadequate Urban Sanitation and Water Management
Rapid urbanisation without resilient drainage systems leads to frequent waterlogging, contaminating potable water and triggering outbreaks of hepatitis A and diarrhoeal diseases.
Example: Case Study – Mumbai Flooding Episodes: Recurrent monsoon flooding has repeatedly overwhelmed sewage systems, leading to spikes in leptospirosis cases, exposing gaps in urban planning-health coordination.
Government efforts like Jal Jeevan Mission and AMRUT aim to improve piped water and sewage systems, but uneven implementation limits outcomes.
Overburdened and Uneven Healthcare Infrastructure
Public health facilities, especially in rural and peri-urban areas, face shortages of beds, trained personnel, and diagnostic capacity, constraining response during seasonal disease surges.
Example: Case Study – Encephalitis and diarrhoeal outbreaks in eastern India show how primary health centres fail to handle sudden case loads.
Schemes such as Ayushman Bharat (Health and Wellness Centres) seek decentralised care but remain under-resourced in climate-sensitive zones.
Weak Surveillance and Early Warning Systems
Disease monitoring systems often lack real-time data integration, delaying response to outbreaks linked to climate variability.
Example: Delayed detection of dengue pattern shifts in Delhi-NCR, where peak incidence has shifted due to prolonged warm conditions.
Initiatives like Integrated Disease Surveillance Programme (IDSP) exist but require technological strengthening and local-level data integration.
2. Climate-Induced Expansion and Intensification of Disease Burden
Changing Epidemiology of Waterborne and Vector-borne Diseases
Erratic rainfall and rising temperatures expand the geographical spread of vectors and pathogens into previously unaffected areas.
Example: Case Study – Malaria in Himachal Pradesh: Traditionally a low-risk area, now reporting cases due to rising temperatures enabling mosquito survival.
The National Vector Borne Disease Control Programme (NVBDCP) is adapting strategies, yet struggles with newly emerging transmission zones.
Heat Stress and Non-Communicable Disease (NCD) Linkages
Extreme heat increases cardiovascular strain, aggravates hypertension, and contributes to kidney diseases due to dehydration.
Example: Heatwave Mortality in Odisha and Telangana demonstrates rising deaths among outdoor workers lacking cooling infrastructure.
Government interventions like National Action Plan on Climate Change (NAPCC) include health adaptation, but implementation remains fragmented.
Air Pollution and Multi-Organ Health Impacts
Increased reliance on cooling systems raises greenhouse gas emissions, elevating PM2.5 levels, which penetrate lungs and bloodstream.
Leads to chronic obstructive pulmonary disease (COPD), atherosclerosis, and kidney dysfunction, compounding heat-related stress.
Example: Urban clusters like Delhi-NCR face simultaneous heatwaves and pollution spikes, creating compound health risks.
The National Clean Air Programme (NCAP) aims to reduce particulate pollution but lacks direct integration with health emergency frameworks.
3. Socio-economic and Governance Constraints Limiting Adaptive Capacity
Vulnerability of Marginalised Populations
Informal workers, slum dwellers, and rural poor lack access to clean water, cooling systems, and healthcare, making them disproportionately affected.
Example: Case Study – Manual Labourers during Heatwaves: High exposure leads to dehydration and heatstroke, often untreated due to wage loss concerns.
Social protection schemes like MGNREGA partially address livelihood stress but are not climate-health integrated.
Food Security, Nutrition and Health Linkages
Climate variability disrupts agriculture, reducing crop yields and nutritional quality, increasing malnutrition and weakened immunity.
Heat stress in livestock reduces milk production, affecting child nutrition.
Example: Unseasonal rainfall impacts on staple crops have led to rising food prices and micronutrient deficiencies in vulnerable populations.
Programs like POSHAN Abhiyaan attempt to address nutrition gaps but are indirectly affected by climate variability.
Policy Fragmentation and Lack of Integrated Health-Climate Governance
Climate change and health policies operate in silos, lacking intersectoral coordination between environment, urban development, and health ministries.
Absence of heat action plans in many regions and limited enforcement where present reduces effectiveness.
Example: Ahmedabad Heat Action Plan is a successful model, yet replication across states remains inconsistent.
Recent policy efforts emphasise climate-resilient health systems, but require stronger institutional convergence and funding.
Conclusion
India’s healthcare system faces a compound crisis where infectious diseases driven by water insecurity intersect with heat-induced non-communicable conditions, exposing systemic gaps in infrastructure, surveillance, and governance.
With projections indicating a sharp rise in heatwave days and climate-sensitive disease burdens by 2030, strengthening climate-resilient healthcare systems, expanding early warning networks, and ensuring equitable access to water, nutrition, and cooling infrastructure become imperative.
A whole-of-government and whole-of-society approach, integrating health into climate policy frameworks, offers a sustainable pathway to mitigate this escalating public health emergency.
Recap: