India’s HIV Epidemic Control Strategy vs TB Eradication Efforts: Key Differences & State-Level Variations Explained
India’s HIV epidemic control strategy and its current TB eradication efforts represent two contrasting public health journeys shaped by institutional design, disease characteristics, and State-level variations. While India managed to reduce HIV prevalence through targeted interventions and autonomous bodies, tuberculosis continues to remain the country’s largest infectious disease burden due to its airborne spread, latent load, and systemic health infrastructure challenges.
Introduction
- The control of communicable diseases in India has historically been shaped by the scale of epidemics, strength of public health systems, and responsiveness of government interventions. HIV/AIDS, caused by the Human Immunodeficiency Virus, emerged as a major public health threat in the late 1980s and early 1990s, with many countries facing adult prevalence rates in double digits and very high mortality due to lack of treatment.
- India’s adult prevalence remained below 1%, yet its spread across almost all States made it a major national concern. In contrast, tuberculosis (TB) continues to be India’s largest infectious disease burden, with India currently accounting for about one-fourth of the global TB caseload and similar proportions of global multidrug-resistant TB cases.
- While India contributes around 7–8% of people living with HIV globally, its TB burden is disproportionately higher, highlighting the scale of challenges involved in eradication. Both diseases exhibit overlaps, particularly through HIV-TB co-infection, but the strategies, institutional frameworks, pace of decline, and State-level outcomes differ significantly.
1. Strategic Design and Institutional Architecture
1.1 Program Structure and Autonomy
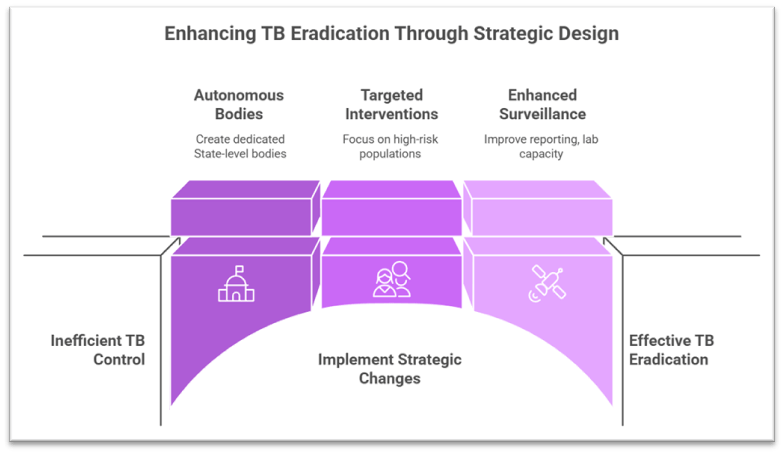
- HIV control strategy evolved through the creation of autonomous and dedicated State-level implementing bodies such as the State AIDS Control Societies (SACS), first pioneered in Tamil Nadu. These bodies enabled direct fund flow, operational flexibility, targeted interventions, and strong coordination with civil society organisations.
- Example: TNSACS model enabling rapid awareness campaigns and behavioural change interventions.
- TB eradication efforts, under the National TB Elimination Programme (NTEP), are embedded largely within the general health system. While they have strong vertical components, they lack the same degree of autonomy seen in AIDS control efforts due to the heavy dependence on existing public health infrastructure.
- HIV control benefitted from early international financing support, providing clear programmatic direction. TB efforts rely more on domestic funding supplemented by multilateral agencies, but the scale of implementation within the health system creates bureaucratic delays, especially in high-burden States.
1.2 Nature of Interventions
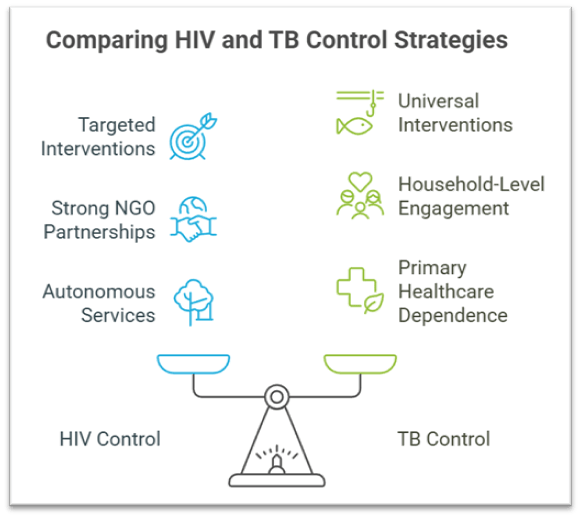
- HIV control relied heavily on awareness generation, stigma reduction, condom promotion, behavioural change communication, and later on free antiretroviral therapy (ART) once treatment became available. These interventions were community-based and focused on targeted populations such as truck drivers, sex workers, and injecting drug users.
- TB control requires active case finding, microbiological confirmation (CB-NAAT/TrueNat), treatment initiation, nutritional support, and rigorous follow-up. Strategies must address latent TB, multidrug-resistant TB, and socio-economic determinants like poor nutrition.
- The HIV epidemic plateaued early due to behavioural change and prevention measures, whereas TB elimination demands continuous surveillance, given its airborne spread and high reinfection vulnerability.
1.3 Monitoring, Surveillance, and Reporting
- HIV surveillance combines sentinel surveillance, targeted intervention reporting, behavioural surveillance, and ART programme data, enabling stable long-term prevalence estimates and rapid response strategies.
- TB surveillance has significantly improved after making TB a notifiable disease, but remains heavily dependent on the quality of State-level reporting, laboratory capacity, and private-sector compliance.
- Example: Introduction of Nikshay portal for real-time TB surveillance.
- HIV control shows stable or declining prevalence in most States, while TB surveillance continues to reveal high hidden caseloads in densely populated northern States due to gaps in active detection.
2. Operational Challenges and Program Delivery
2.1 Availability of Treatment and Technological Capacity
- In the early HIV response, there was no curative treatment, making prevention the core strategy. Once ART became accessible, it improved survival and reduced infectivity, contributing to overall prevalence reduction.
- TB eradication depends on timely access to drug-sensitive TB regimens, MDR-TB treatment, and diagnostics. The complexity of treatment (6 months for drug-sensitive TB, 18–24 months for MDR-TB) and side-effects leads to high default rates, especially in vulnerable populations.
- States with strong public health systems like Tamil Nadu, Kerala, and Himachal Pradesh have integrated AI-based predictive tools, rapid molecular diagnostics, and better treatment adherence mechanisms.
- Example: Introduction of predictive mortality-risk models in Tamil Nadu’s TB programme.
2.2 Community Engagement and Behavioural Dimensions
- HIV control involved strong partnerships with NGOs, community-based organisations, and peer educators, which helped address stigma and expand testing among high-risk groups.
- TB control requires household-level engagement, counselling for treatment adherence, and nutritional support schemes such as Ni-kshay Poshan Yojana. However, social stigma and lack of community-based support in high-burden districts impede detection and adherence.
- HIV programme success was driven by targeted interventions, while TB eradication needs universal interventions due to the airborne nature of transmission, thereby increasing programmatic load.
2.3 Integration with General Health Systems
- Over time, HIV services became well-integrated through ART centres, ICTC centres, and district-level units, yet continued to operate with a high degree of autonomy.
- TB control is deeply embedded in primary healthcare, requiring coordination from sub-centres to district hospitals. The dependence on routine health machinery means that systemic weaknesses directly affect TB outcomes, particularly in States with staff shortages or limited laboratory capacity.
- Integration is further complicated by HIV-TB co-infection, requiring coordinated case management across both programmes, especially in urban slums and tribal areas.
3. State-Level Variations and Impact on Outcomes
3.1 Disproportionate Disease Burden across States
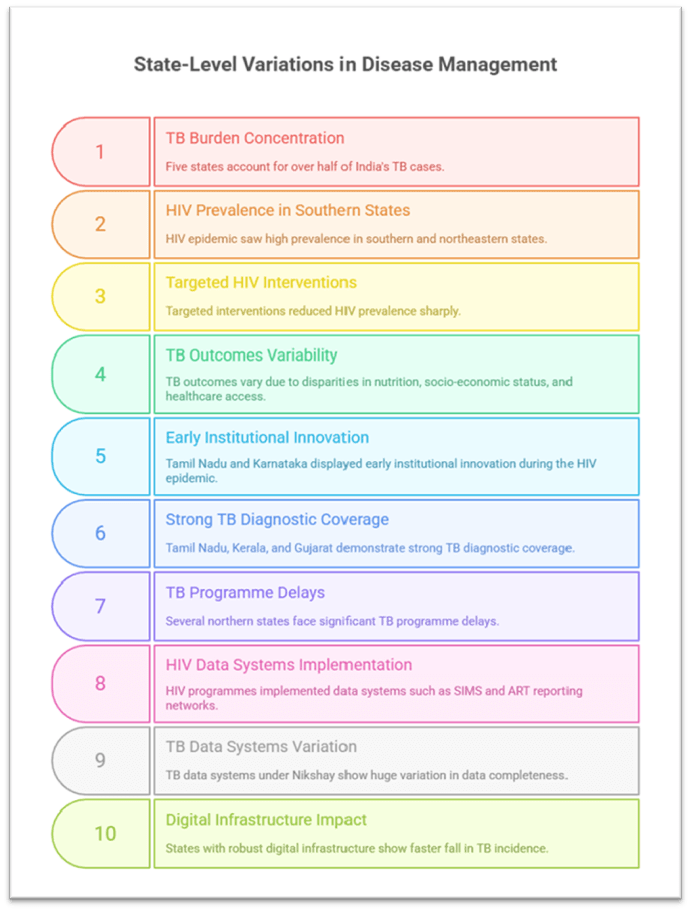
- TB burden is highly concentrated: Five States (Uttar Pradesh, Maharashtra, Madhya Pradesh, Bihar, Rajasthan) account for over half of India’s TB cases. These are also States with weaker health indicators, lower public health spending, and high population density.
- In contrast, the HIV epidemic saw high prevalence in southern States and certain northeastern States, but targeted interventions using autonomous agencies reduced prevalence sharply.
- Variability in TB outcomes mirrors disparities in nutrition levels, socio-economic status, and access to healthcare, unlike HIV, where behavioural interventions led to more uniform decline.
3.2 Differences in Institutional Responsiveness
- States like Tamil Nadu and Karnataka displayed early institutional innovation during the HIV epidemic, improving program delivery, surveillance, and awareness campaigns.
- In TB control, Tamil Nadu, Kerala, and Gujarat demonstrate strong diagnostic coverage, adoption of new technologies, and better treatment adherence, whereas several northern States face significant programme delays.
- State capacity, including supply chain efficiency, staffing levels, and local governance, determines TB outcomes far more than HIV outcomes due to the higher operational intensity of TB control.
3.3 Adoption of Technology and Data Systems
- HIV programmes implemented data systems such as SIMS and ART reporting networks, standardised across States.
- TB data systems under Nikshay show huge variation in data completeness, private-sector reporting, and follow-up.
- Example: Tamil Nadu’s integration of ICMR-developed mortality-prediction software enhances timely intervention, not yet replicated uniformly across the country.
- States with robust digital infrastructure show faster fall in TB incidence, while others struggle with data gaps, impacting national progress.
Conclusion:
- India’s experience with HIV control represents a successful public health response built on autonomous institutions, targeted interventions, strong surveillance, and behaviour-based prevention strategies, leading to a reduction in adult HIV prevalence from over 0.5% to about 0.22% today.
- TB eradication, however, faces a far more complex challenge due to the airborne nature of transmission, high latent burden, MDR-TB, and dependence on the general health system. State-level differences in institutional capacity, diagnostics, socio-economic vulnerabilities, and governance structures substantially influence outcomes, making uniform national progress difficult.
- With India accounting for one-fourth of global TB cases, achieving TB eradication requires a sharper focus on State-specific strategies, mirroring the adaptive and decentralised approach that proved effective in HIV control. A combination of strong political commitment, technology-enabled surveillance, and community-centred care can help accelerate India’s progress towards national and global TB elimination goals.
- India’s experience with HIV control represents a successful public health response built on autonomous institutions, targeted interventions, strong surveillance, and behaviour-based prevention strategies, leading to a reduction in adult HIV prevalence from over 0.5% to about 0.22% today.
- TB eradication, however, faces a far more complex challenge due to the airborne nature of transmission, high latent burden, MDR-TB, and dependence on the general health system. State-level differences in institutional capacity, diagnostics, socio-economic vulnerabilities, and governance structures substantially influence outcomes, making uniform national progress difficult.
- With India accounting for one-fourth of global TB cases, achieving TB eradication requires a sharper focus on State-specific strategies, mirroring the adaptive and decentralised approach that proved effective in HIV control. A combination of strong political commitment, technology-enabled surveillance, and community-centred care can help accelerate India’s progress towards national and global TB elimination goals.
Recap: