

Introduction:
- Healthcare access refers to the ability of individuals and communities to obtain timely, affordable, acceptable and quality health services without suffering financial hardship. It constitutes the foundation of Universal Health Coverage (UHC), a core component of the Sustainable Development Goals. Despite significant improvements in life expectancy, immunization coverage and disease control, India continues to face substantial healthcare access deficits.
- While public health expenditure has increased in recent years and initiatives such as Ayushman Bharat, National Health Mission, and the Ayushman Bharat Digital Mission have expanded the healthcare landscape, a large proportion of households continue to incur catastrophic health expenditure, revealing a disconnect between policy priorities and people’s immediate healthcare needs. Reconnecting public health with citizens’ lived realities requires strengthening healthcare delivery systems, addressing social determinants, and ensuring equitable, people-centric health governance.
Body:
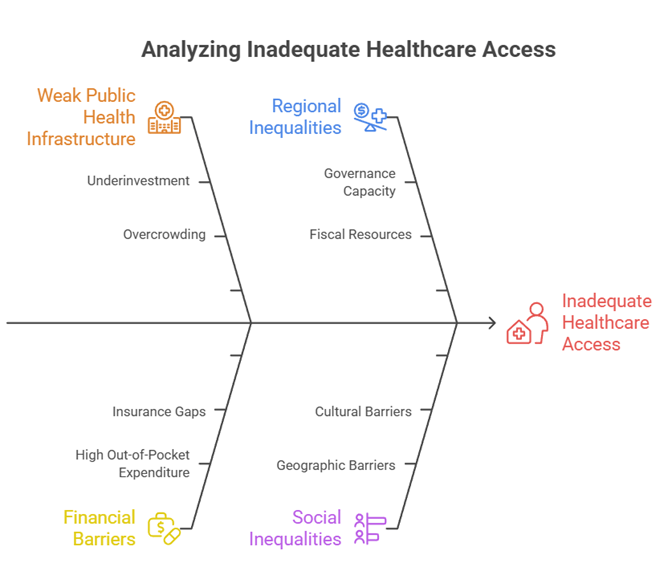
I. Structural Factors Responsible for Inadequate Access to Healthcare
1. Weak Public Health Infrastructure and Human Resource Gaps
- Persistent underinvestment in primary healthcare has resulted in shortages of doctors, nurses, specialists, diagnostic facilities and essential medicines, particularly in rural, tribal and aspirational districts, limiting timely access to care.
- Large sections of the population continue to depend on overcrowded public hospitals where inadequate infrastructure, equipment shortages and long waiting times reduce the quality of care and discourage utilization.
- Example – Rural Health Service Gaps: Several remote districts in states such as Jharkhand, Chhattisgarh and Odisha continue to face specialist vacancies in Community Health Centres, forcing patients to travel long distances for basic treatment.
2. Financial Barriers and High Out-of-Pocket Expenditure
- Despite the expansion of publicly funded insurance schemes, healthcare financing remains heavily dependent on household expenditure, especially for medicines, diagnostics and outpatient care.
- Insurance-based models often focus on hospitalization while neglecting routine consultations, chronic disease management and preventive services, resulting in continued financial vulnerability.
- Case Study – Catastrophic Health Expenditure: Numerous studies have shown that serious illnesses such as cancer, cardiovascular diseases and kidney disorders continue to push vulnerable households into debt despite insurance coverage due to indirect costs and uncovered treatments.
3. Regional, Social and Urban-Rural Inequalities
- Healthcare access remains uneven across states due to differences in governance capacity, fiscal resources and health infrastructure development.
- Marginalized groups including women, Scheduled Tribes, migrant workers, urban poor and persons with disabilities often face geographic, cultural and informational barriers in accessing healthcare services.
- Example – Tribal Health Challenges: Tribal populations in central Indian regions continue to experience higher burdens of malnutrition, maternal mortality and communicable diseases because of difficult terrain and inadequate service delivery.
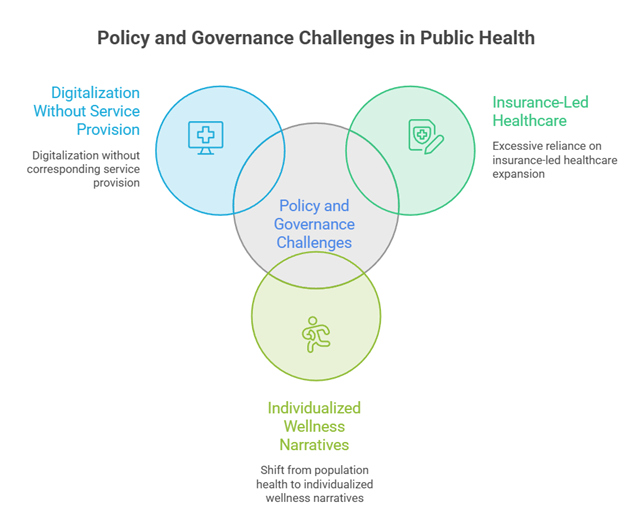
II. Policy and Governance Challenges Creating a Disconnect Between Public Health and People’s Needs
1. Excessive Reliance on Insurance-Led Healthcare Expansion
- Publicly funded insurance has improved access to selected tertiary-care procedures but often diverts attention from strengthening foundational public health institutions such as Sub-Centres, Primary Health Centres and Community Health Centres.
- Package-based reimbursement systems may create incentives for unnecessary procedures, over-medicalization and profit-driven healthcare practices rather than comprehensive patient care.
- Example – Investigations into Unnecessary Procedures: Instances of allegedly unwarranted medical interventions under insurance reimbursement systems have raised concerns regarding regulation and accountability.
2. Shift from Population Health to Individualized Wellness Narratives
- Contemporary policy discourse increasingly emphasizes wellness, lifestyle modification and behavioural choices, sometimes overlooking structural determinants such as poverty, nutrition, sanitation, housing and environmental conditions.
- Health outcomes are strongly shaped by socioeconomic realities; therefore, expecting individuals alone to achieve wellness without supportive environments may widen inequalities.
- Case Study – Non-Communicable Diseases: Rising diabetes and hypertension prevalence demonstrates that individual behavioural interventions alone cannot substitute for healthier food systems, urban planning and preventive public health measures.
3. Digitalization Without Corresponding Service Provision
- Digital health platforms improve record management, portability and administrative efficiency but cannot substitute for the physical availability of doctors, medicines, laboratories and hospitals.
- Technological solutions often face challenges of digital literacy, connectivity gaps and exclusion among elderly, rural and vulnerable populations.
- Example – Digital Health Ecosystem: The creation of digital health identities and registries can facilitate continuity of care, but their effectiveness depends on the existence of functioning healthcare facilities capable of delivering services.
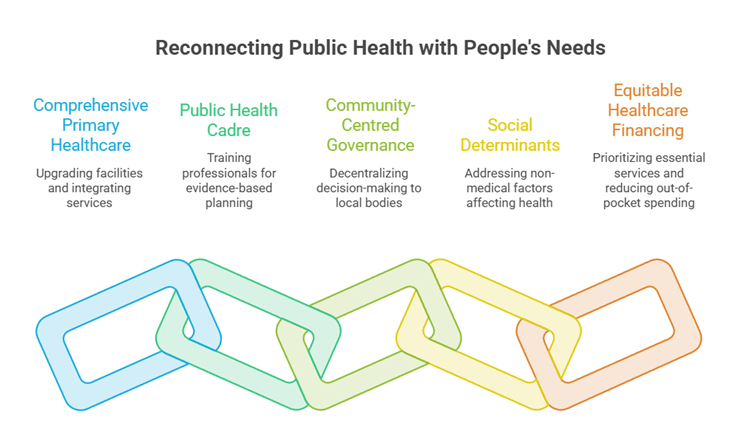
III. Measures to Reconnect Public Health with People’s Felt Needs
1. Strengthen Comprehensive Primary Healthcare and Public Institutions
- Public investment should prioritize upgrading Sub-Centres, Primary Health Centres and Community Health Centres through improved infrastructure, diagnostics, essential drug availability and adequate staffing.
- Healthcare systems should focus on people’s immediate curative needs while simultaneously integrating preventive, promotive and rehabilitative services.
- Government Initiative – Ayushman Arogya Mandirs: The transformation of primary healthcare facilities into comprehensive care centres can become effective when supported by sufficient manpower, medicines and referral systems.
2. Establish a Robust Public Health Cadre and Community-Centred Governance
- A dedicated interdisciplinary public health cadre trained in epidemiology, health management, environmental health and community engagement can improve evidence-based planning and implementation.
- Decentralized governance involving local bodies, community organizations and frontline health workers can ensure that policies reflect local health priorities and cultural contexts.
- Case Study – Kerala’s Community-Based Public Health Model: Strong local governance, public participation and primary healthcare networks have contributed to better health indicators and effective disease surveillance.
3. Address Social Determinants and Ensure Equitable Healthcare Financing
- Sustainable improvements in health require coordinated action on nutrition, sanitation, drinking water, housing, education, gender equality and environmental protection.
- Public financing should prioritize essential healthcare services and reduce dependence on out-of-pocket spending through strengthened public provisioning and affordable medicines.
- Government Initiatives – POSHAN Abhiyaan, Jal Jeevan Mission and Swachh Bharat Mission: These programmes illustrate how non-medical interventions directly influence health outcomes by reducing malnutrition, infectious diseases and environmental health risks.
Conclusion:
- India’s healthcare challenge is not merely one of financing or technology but of aligning public health systems with the everyday realities of its people. Genuine progress toward Universal Health Coverage requires moving beyond fragmented and insurance-centric approaches toward a resilient public health architecture rooted in accessible primary care, social justice and community participation.
- As India advances toward becoming a developed nation, strengthening public healthcare institutions, addressing social determinants and ensuring equitable access can transform health from a service that people struggle to obtain into a fundamental guarantee that enhances human development, productivity and national well-being.
