Introduction
• Tuberculosis remains one of India’s most persistent public health challenges, accounting for nearly one-fourth of the global TB burden. Despite decades of programme-based control, gaps in early diagnosis, drug-resistance management, nutritional vulnerability, and treatment adherence continue to impede India’s National TB Elimination Programme (NTEP) from reaching the target of Ending TB by 2025.
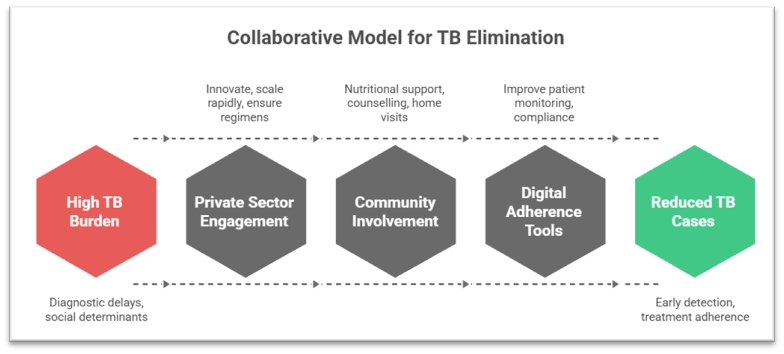
• In this context, a collaborative model that integrates the strengths of government systems, private innovators, and community health workers has emerged as a necessity rather than an option. With India reporting millions of cases annually and a significant share of rifampicin-resistant TB going undetected until recent years, the integration of point-of-care molecular diagnostics, digital adherence tools, public–private partnerships, and decentralised community outreach has demonstrated measurable improvements in detection and treatment metrics.
Body
1. Necessity of a Collaborative Model for TB Elimination in India
1.1 Addressing Diagnostic Delays and Infrastructure Constraints
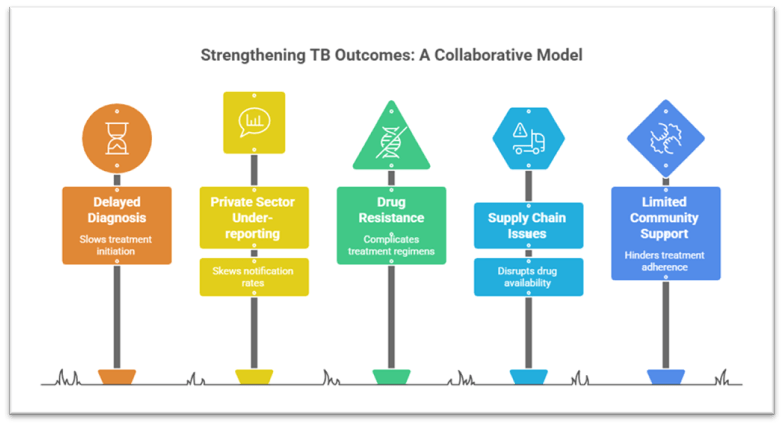
. Inadequate early detection capacity remained a major barrier under traditional sputum microscopy, which had low sensitivity, especially among children, people with HIV, and extrapulmonary TB cases. Deployment of portable molecular diagnostics, supported by private innovators, enabled under-one-hour detection, reducing dependency on centralised labs.
Example: Truenat-based decentralised testing increased detection of rifampicin-resistant TB in countries where India’s technology was scaled.
. Government health system limitations such as uneven diagnostic coverage in tribal belts, conflict areas, and remote districts made it essential to involve private diagnostic manufacturers that could innovate and scale rapidly.
Example: Over 4000+ point-of-care molecular systems deployed under NTEP significantly reduced the time between suspicion and treatment initiation.
. High paediatric diagnostic challenges, especially due to the difficulty of sputum collection, necessitated innovations like stool-based molecular testing validated in African primary healthcare settings and piloted in India for child TB detection.
Schemes: Paediatric TB management strengthened under the Nikshay Poshan Yojana and Paediatric TB Management Guidelines emphasising early diagnosis.
1.2 Combating Social Determinants: Malnutrition, Poverty, and Stigma
. Malnutrition contributes to about 40% of TB in India, and this cannot be resolved by health systems alone. Community health workers and civil society organisations play a critical role in linking nutritional support with treatment pathways.
Scheme: Nikshay Poshan Yojana provides monthly nutritional support to TB patients via DBT.
. Stigma and misinformation often prevent timely health-seeking behaviour, especially among migrant workers and women. Community volunteers, self-help groups, and TB champions help bridge these behavioural and social gaps through counselling and home visits.
Example: Community-led TB campaigns in Rajasthan and Maharashtra improved treatment adherence.
. Economic burden on households, given the long treatment period, demands convergence between government social protection schemes, private CSR initiatives, and local support networks to ensure continuity of care.
Schemes: Ayushman Bharat, Pradhan Mantri Jan Arogya Yojana (PMJAY), and community-based livelihood schemes reduce catastrophic health expenditures.
1.3 Need to Manage Drug Resistance and Strengthen Treatment Adherence
. India contributes significantly to global MDR-TB cases, and improper treatment adherence is one of the major drivers. Private sector engagement helps ensure standardised regimens, real-time reporting, and drug-resistance surveillance.
Example: Expansion of Line Probe Assay labs and molecular platforms through public–private financing.
. Digital adherence tools, many developed by private innovators, such as 99DOTS and electronic pillboxes, improve patient monitoring but require community health workers for field-level implementation.
Scheme: Nikshay Mitra (Pradhan Mantri TB Mukt Bharat Abhiyan) integrates community adoption and private support.
. Complex treatment regimens necessitate integrated models where government oversight ensures protocol adherence, innovators supply technology, and frontline workers ensure daily compliance through home-based care.
2. Efficacy of the Collaborative Model in Strengthening TB Outcomes
2.1 Improved Case Detection, Timely Diagnosis, and Faster Treatment Initiation
. Point-of-care molecular diagnostics have substantially narrowed the gap between suspicion and treatment initiation. Trials in African primary health centres demonstrated significantly higher treatment initiation within seven days, a pattern replicated in several Indian districts where decentralised testing was adopted.
. Government–private procurement partnerships enabled rapid scale-up of indigenous diagnostics, minimising reliance on imported systems and reducing costs, making India’s TB programme more resilient and self-sustaining.
. Mobile diagnostic units supported by NGOs and startups in hard-to-reach geographies improved active case finding among nomadic communities and tribal populations, increasing notification rates under NTEP.
2.2 Strengthened Surveillance, Monitoring, and Drug-Resistance Management
. Nikshay portal integration, supported by private software solutions and health workers’ real-time field inputs, significantly improved notification rates from the private sector, which was previously under-reporting TB cases.
Result: Over 1.8 million private sector notifications annually in recent years.
. Robust drug-resistance surveillance, enabled by private sector technology, allows faster shifts to appropriate regimens, improving outcomes in MDR/XDR-TB patients.
Example: Introduction of shorter MDR-TB regimens validated globally.
. Better supply-chain management, facilitated by digital innovations and government procurement reforms, ensures uninterrupted availability of TB drugs even in remote blocks.
2.3 Enhanced Community Engagement and Treatment Adherence
. Community health workers, including ASHAs and TB champions, have increased treatment completion rates by providing doorstep support, bridging gaps between clinics and households.
Example: Community engagement models in Bihar and Uttar Pradesh led to improved adherence among migrant workers.
. Civil-society–government convergence under the TB Mukt Gram Panchayat initiative supports local surveillance, awareness drives, and nutritional basket support, strengthening decentralised responses.
. Private CSR partnerships have helped deliver food baskets, diagnostics subsidies, and workplace TB screening, making adherence and prevention socially integrated rather than clinic-dependent.
3. Remaining Challenges and the Need for Strengthening the Collaborative Model
3.1 Persistent Social Inequalities and High Determinants of Vulnerability
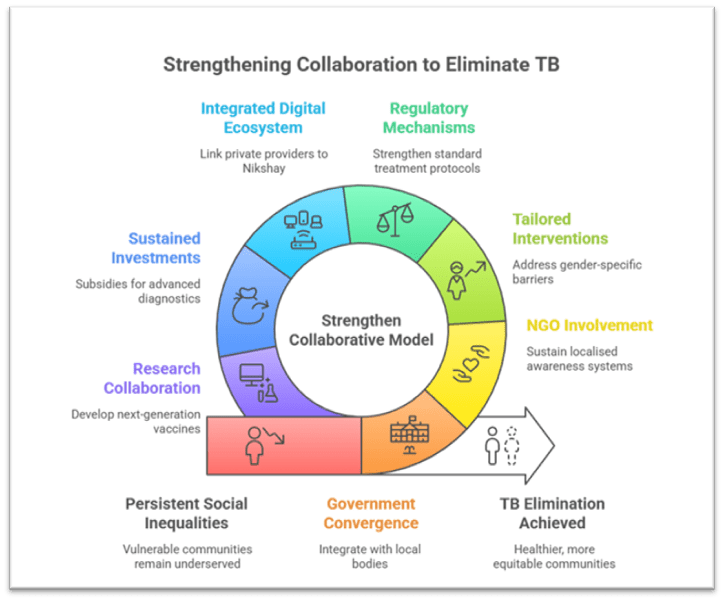
. Undernutrition, overcrowding, and poor sanitation continue to fuel TB incidence, demanding deeper government convergence with urban local bodies, rural development schemes, and CSR nutrition programmes.
. Marginalised communities remain underserved despite progress, necessitating greater involvement from grassroots NGOs to sustain localised awareness and support systems.
. Gender-specific barriers, particularly for women domestic workers and homemakers, require tailored interventions involving self-help groups and local women’s collectives.
3.2 Variability in Private Sector Quality and Standardisation
. Unregulated private prescriptions and irrational use of antibiotics persist in some areas, undermining TB elimination efforts. Strengthening standard treatment protocols through collaborative regulatory mechanisms is essential.
. Uneven adoption of digital tools in the private sector hinders uniform reporting. A more integrated digital ecosystem linking all private providers to Nikshay is necessary.
. Procurement and cost variations for advanced diagnostics still pose issues despite improved indigenous innovation, highlighting the need for sustained investments and subsidies.
3.3 Need for Greater Research, Innovation, and Integrated Public Health Interventions
. Next-generation vaccines, improved MDR-TB drugs, and simplified oral regimens require collaboration between government research bodies and private biotech firms.
. Integration with nutrition, mental health, and social protection services remains incomplete; community workers alone cannot address systemic gaps without interdepartmental coordination.
. Urban TB transmission, especially in slums, demands stronger partnerships with municipal bodies, resident welfare associations, and urban primary healthcare networks.
Conclusion
• A high-burden country like India cannot eliminate TB without a robust multi-stakeholder ecosystem that combines the reach of government systems, the agility and innovation of private enterprises, and the community-level trust and continuity provided by health workers. Evidence from India and comparable global settings shows that such a collaborative model leads to faster diagnosis, higher treatment adherence, improved drug-resistance management, and greater social protection coverage.
• As TB remains deeply rooted in inequality, the way forward lies in sustained investment in indigenous diagnostics, integration of nutrition and social welfare schemes, acceleration of vaccine research, expansion of community-led surveillance, and universal adoption of digital tools. With strengthened coordination and continuous innovation, India can transform its high burden into an opportunity for global leadership in public health and move decisively toward its TB elimination goals.
Recap: