How Public–Private Partnerships in Indian Healthcare Threaten Public Health & the Right to Health
Public–Private Partnerships in Indian Healthcare have expanded rapidly in recent years, raising critical concerns about accessibility, affordability, and the weakening of public health systems. A robust public health system is central to the realization of health as a fundamental human right, a principle echoed in India’s constitutional values and international commitments. However, India’s health system continues to grapple with chronic underfunding, with public expenditure hovering around 1.2% of GDP and only about 2% of the Union Budget allocated to health. Annual public spending remains low at around USD 25 per capita, resulting in a fragile infrastructure heavily relied upon by nearly 80 crore people. Against this backdrop, the rapid expansion of public–private partnerships (PPPs) and the commercialisation of health care has raised critical questions about affordability, accessibility, and equity. The debate centres on whether these trends strengthen service delivery or risk further eroding an already strained public health system, ultimately determining the extent to which health can meaningfully function as a fundamental right.
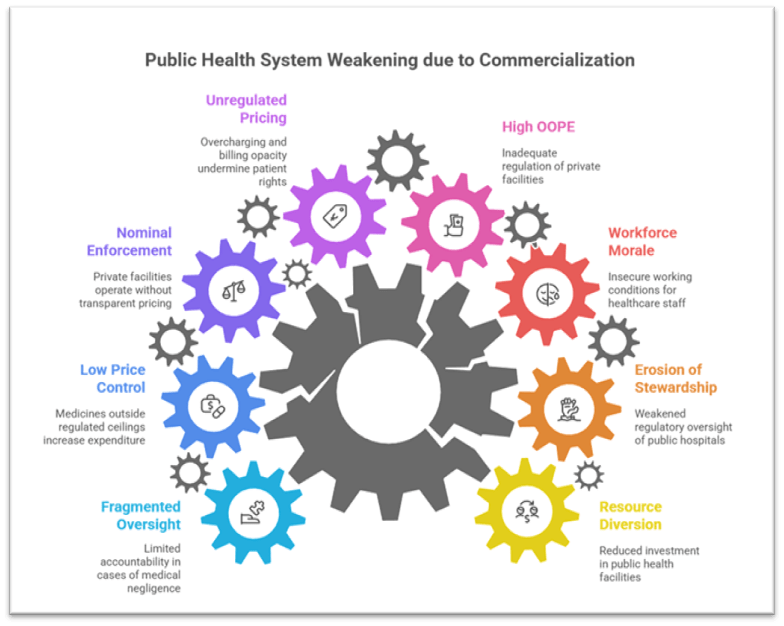
Risks Posed by Commercialisation to Public Health Systems
1. Weakening of Public Infrastructure
- Diversion of resources to private players often leads to reduced investment in government facilities, especially district hospitals and primary health centres, limiting public capacity to serve the poorest.
Example: The PPP medical college model in several States resulted in private partners controlling clinical facilities, leading to prioritisation of revenue over service delivery. - Erosion of government stewardship occurs when administrative control of public hospitals shifts towards private entities, weakening regulatory oversight.
Case Study: The experience in Andhra Pradesh’s PPP hospitals, where cost escalation and reduced access for low-income families were observed. - Loss of workforce morale as contractualisation and outsourcing under PPPs create insecure working conditions for nurses, ASHAs and paramedical staff.
Government Initiative: The National Health Mission (NHM) attempts to strengthen staffing but struggles against contractual PPP practices.
2. Affordability Concerns and Rising Financial Burden
- High out-of-pocket expenditure (OOPE) persists, accounting for nearly half of total health spending, partly due to inadequate regulation of private facilities.
Example: The high rates for caesarean sections in corporate hospitals despite regulatory norms. - Unregulated pricing practices such as overcharging, billing opacity and unnecessary procedures undermine patient rights.
Case Study: Several audits under the Clinical Establishments Act exposed steep pricing disparities. - Insurance schemes disproportionately benefit private hospitals, with government-supported schemes used for high-cost tertiary care rather than strengthening primary care.
Initiative: Ayushman Bharat - PM-JAY has been criticised for directing public funds to private hospitals rather than infrastructure upgrades.
3. Regulatory Challenges and Patient Safety Risks
- Nominal enforcement of the Clinical Establishments Act allows private facilities to operate without transparent pricing or adherence to patient rights.
Example: Reports of irrational drug combinations and aggressive marketing practices. - Low price control coverage, with more than 80% of medicines outside regulated ceilings, increases household expenditure.
Government Mechanism: The National Pharmaceutical Pricing Authority (NPPA) struggles to curb excessive markups. - Fragmented oversight frameworks limit accountability in cases of medical negligence or denial of care.
Case Study: Instances of private hospitals refusing treatment during the COVID-19 peak highlighted regulatory gaps.
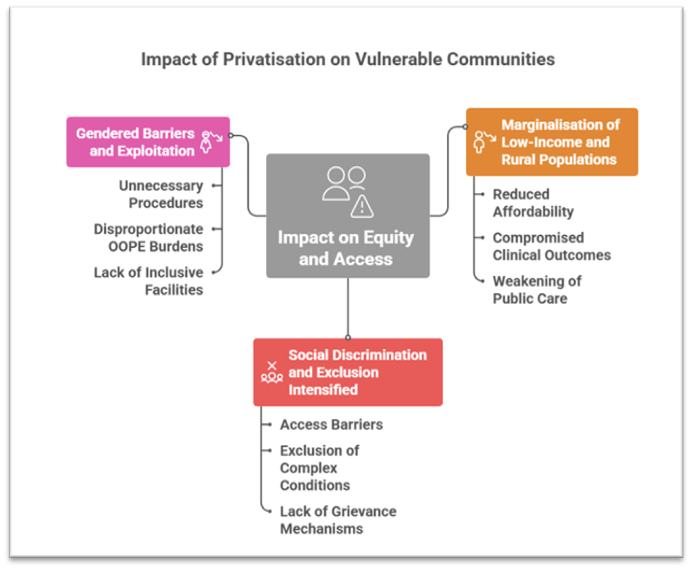
Impact on Equity and Access for Vulnerable Communities
1. Marginalisation of Low-Income and Rural Populations
- Privatisation disproportionately affects rural and tribal regions, where private facilities are scarce and public hospitals are lifelines.
Case Study: Tribal districts in Gujarat experienced reduced affordability for routine services after PPP takeovers. - Increased dependence on informal providers leads to compromised outcomes in underserved communities.
Example: High reliance on unqualified practitioners in eastern States. - Weakening of public preventive and primary care widens health disparities.
Initiative: Health and Wellness Centres aim to mitigate this but remain unevenly implemented.
2. Social Discrimination and Exclusion Intensified
- Social hierarchies manifest in access barriers, especially for Dalits, Adivasis, LGBTQ+ persons and persons with disabilities.
Example: Documented discrimination in private hospitals against transgender individuals. - Commercialised care models often exclude complex or chronic conditions that offer low profit margins.
Case Study: Limited private sector engagement in disability care and mental health services. - Lack of accessible grievance redress mechanisms exacerbates inequity.
Government Attempt: The Charter of Patients’ Rights remains largely voluntary.
3. Gendered Barriers and Exploitation
- High rates of unnecessary procedures such as caesarean sections reflect revenue-driven practices.
Example: Private hospital C-section rates are more than double WHO norms in several States. - Women in informal jobs bear disproportionate OOPE burdens, impacting maternal and reproductive health.
Initiative: Janani Suraksha Yojana (JSY) improves institutional deliveries but cannot offset high private costs. - Lack of inclusive facilities reduces access for women from marginalised groups.
Case Study: Urban health clinics in Delhi and Mumbai struggle to serve migrant women effectively.
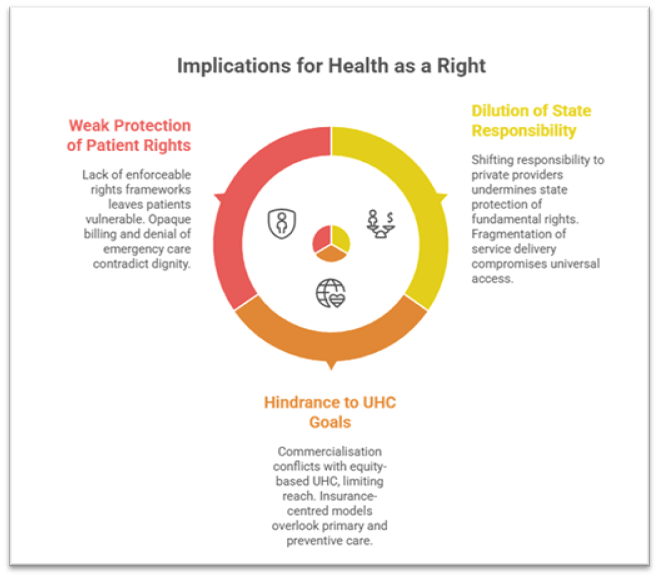
Implications for Health as a Fundamental Right
1. Dilution of State Responsibility
- Excessive reliance on private providers shifts responsibility away from government.
Example: During COVID-19, dependence on private oxygen supplies exposed structural weaknesses. - Fragmentation of service delivery under PPPs undermines universal access and uniform service quality.
Initiative: National Health Policy 2017 emphasises universality, but PPP expansion risks inconsistent implementation. - Reduced public accountability compromises constitutional mandates on equality and social justice.
2. Hindrance to Universal Health Coverage (UHC) Goals
- Commercialisation conflicts with equity-based UHC, as expensive care models limit reach.
Example: Private hospitals cluster in profitable urban zones, leaving rural regions underserved. - Insurance-centred models overlook primary and preventive care.
Government Model: NUHM attempts primary care strengthening but is overshadowed by tertiary insurance schemes. - High OOPE contradicts UHC principles, preventing health from being treated as a right rather than a commodity.
3. Weak Protection of Patient Rights
- Lack of enforceable rights frameworks leaves patients vulnerable to exploitation.
Case Study: Multiple instances of hospitals withholding bodies over unpaid bills. - Opaque billing and denial of emergency care contradict principles of dignity and equality.
- Insufficient regulatory oversight undermines guarantees under Articles 14 and 21.
Conclusion:
The growing trend of public–private partnerships and commercialisation within India’s health sector presents a complex challenge: while private players can contribute capacity, unregulated expansion amid chronic underinvestment threatens to further weaken public health systems relied upon by millions. This trend risks undermining the realisation of health as a fundamental right, particularly for vulnerable groups who depend on equitable and affordable services. Strengthening public financing to at least 2.5% of GDP, ensuring stringent regulation, integrating community-led models, expanding public sector medicine production, and adopting a robust rights-based legislation can collectively safeguard health as an accessible, inclusive and accountable entitlement. A balanced approach that reinforces public systems while ensuring responsible private sector participation is essential for building a resilient and rights-oriented health ecosystem for the decade ahead.
Recap: