Primary Healthcare Centres in Rural India & the Impact of Caregiver Burnout on Healthcare Outcomes
Introduction
Primary Healthcare Centres (PHCs) in rural India form the first formal point of contact between rural populations and the public health system. Established under the Bhore Committee vision (1946), PHCs are designed to provide comprehensive, preventive, promotive, and curative care at the grassroots.
A typical PHC caters to around 30,000 people in plains and 20,000 in hilly or tribal areas, acting as the backbone of rural health delivery. With India having over 25,000 PHCs (Rural Health Statistics, 2023), their reach is unmatched.
However, the dual challenge of rising patient load and caregiver burnout in healthcare undermines the system’s efficiency. Addressing these challenges is crucial for achieving Universal Health Coverage (SDG 3.8) and the objectives outlined in the National Health Policy, 2017.
I. Role of Primary Health Centres in Rural India
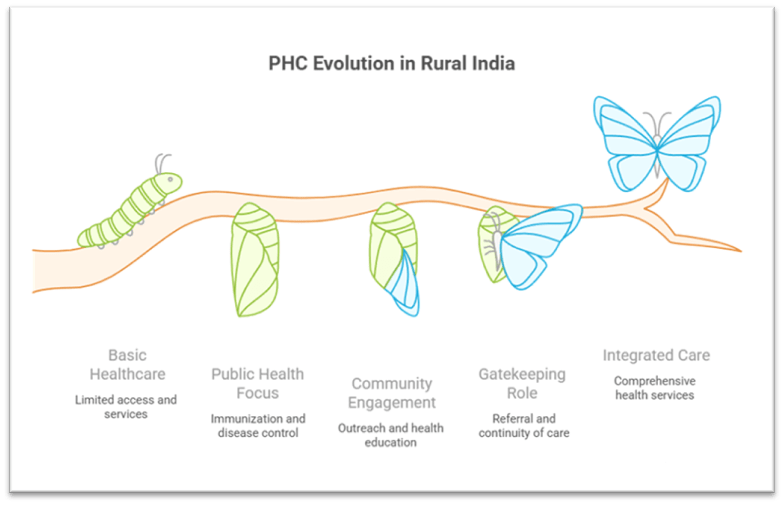
1. Accessibility and Equitable Healthcare
- PHCs ensure geographical and financial access to essential health services for rural and marginalized populations.
- They reduce dependence on tertiary hospitals by offering outpatient care, maternal health, and chronic disease management.
- Example: Tamil Nadu’s NQAS-certified PHCs demonstrate how accessible services improve institutional deliveries and reduce maternal mortality.
2. Public Health and Preventive Services
- PHCs coordinate immunization drives, vector control, and school health programmes at the grassroots level.
- They are crucial for disease surveillance and outbreak response, forming the first reporting point under IDSP.
- Example: During the COVID-19 pandemic, PHCs played a key role in vaccination drives, rural testing, and awareness campaigns.
3. Community Engagement and Social Mobilization
- PHC doctors engage with ASHA workers, ANMs, and Anganwadis to strengthen community outreach.
- They promote health education, sanitation drives, and inter-sectoral coordination through gram sabhas.
- Example: Rashtriya Bal Swasthya Karyakram (RBSK) leverages PHCs for school health check-ups, bridging community and policy.
4. Gatekeeping and Continuity of Care
- PHCs act as gatekeepers to higher-level facilities by providing first-line treatment and referring complex cases.
- They ensure continuity of care across life stages – from neonatal care to geriatrics.
- Example: Ayushman Bharat – Health and Wellness Centres (HWCs), upgraded from PHCs, integrate non-communicable disease (NCD) care with traditional services.
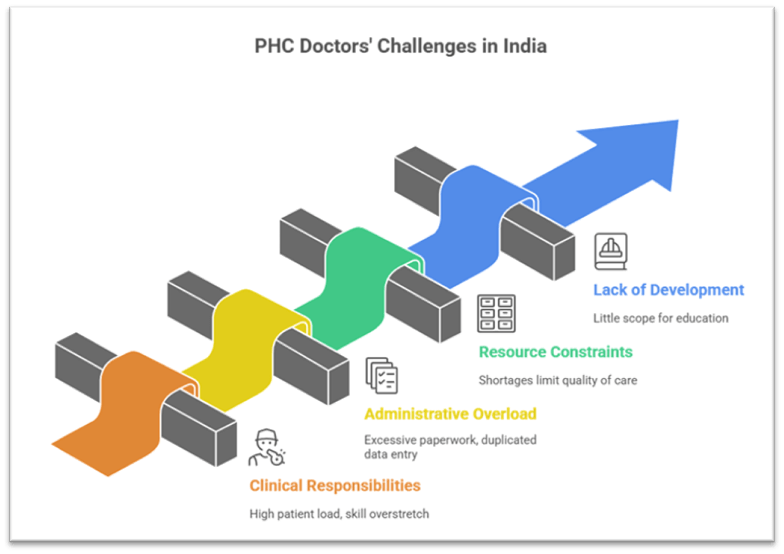
II. Challenges Faced by PHC Doctors
1. Overburdened Clinical Responsibilities
A PHC doctor attends 80–100 patients daily, often handling emergencies without specialist support. They must stay updated across multiple specialties – from paediatrics to psychiatry – leading to skill overstretch.
Example: In remote tribal Jharkhand, PHCs often serve as de facto trauma centres due to the lack of nearby hospitals.
2. Administrative Overload
Doctors maintain over 100 physical registers alongside multiple digital platforms (HMIS, IDSP, IHIP). Duplication of data entry creates a parallel clerical burden, reducing clinical focus.
Example: Despite digitalization efforts under UWIN, many PHCs continue paper-based parallel documentation.
3. Infrastructural and Human Resource Constraints
Many PHCs face shortages of drugs, equipment, and staff nurses, limiting quality of care. Doctor absenteeism, particularly in remote regions, is driven by lack of incentives and living conditions.
Example: Kalahandi district (Odisha) has highlighted gaps in essential medicines and skilled staff in PHCs.
4. Lack of Research and Professional Development
High workload leaves little scope for medical education, reflection, or innovation. Research contributions from PHC doctors, though significant, remain underutilized in policy-making.
Example: Lancet Commission on PHC underscores the need for training, mentorship, and continuous professional development in India.
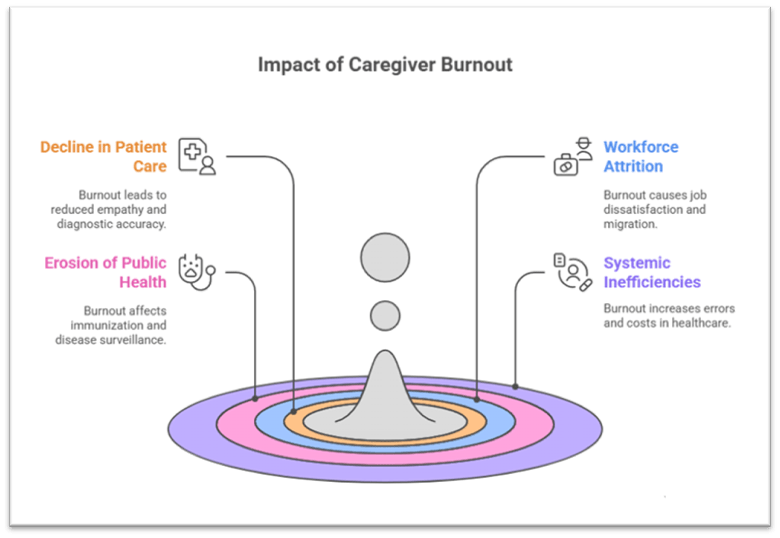
III. Impact of Caregiver Burnout on Healthcare Outcomes
1. Decline in Quality of Patient Care
Burnout causes emotional exhaustion, detachment, and reduced empathy, leading to compromised consultations. High patient volume reduces diagnostic accuracy and patient satisfaction.
Example: WHO Bulletin notes one-third of PHC physicians in LMICs report emotional exhaustion, affecting quality of care.
2. Workforce Attrition and Absenteeism
Burnout fuels job dissatisfaction, absenteeism, and migration to urban/private sectors. Rural areas, already underserved, face a reinforcing cycle of shortages.
Example: Studies from Saudi Arabia’s PHCs show administrative overload as a key driver of physician attrition, a parallel to India’s context.
3. Erosion of Public Health Programmes
Overstressed doctors are less effective in coordinating immunization, disease surveillance, and outreach programmes. Programme-driven targets overshadow patient-centered care, diluting long-term impact.
Example: In regions with high PHC staff burnout, tuberculosis detection under RNTCP has shown delays in case notification.
4. Systemic Inefficiencies and Costs
Burnout increases medical errors, staff turnover, and hidden costs to the system. It reduces trust in public health institutions, pushing people towards out-of-pocket private expenditure.
Example: The National Sample Survey 2019 found nearly two-thirds of rural patients prefer private care, partly due to perceived inefficiency of PHCs.
Conclusion
Primary Healthcare Centres in rural India remain the linchpin of the country’s health architecture, providing both curative and preventive services to millions. Yet, caregiver burnout in healthcare threatens their sustainability, eroding quality, efficiency, and trust in the system.
Addressing this requires systemic reforms: meaningful digitalization to cut duplication, task-shifting of non-clinical work, better incentives for rural service, and focus on physician well-being. Global efforts such as the “25 by 5” campaign to reduce documentation time highlight practical pathways.
With India targeting Universal Health Coverage under SDG 3 and investing in 1.5 lakh Health and Wellness Centres under Ayushman Bharat, strengthening PHCs must begin with protecting those who hold them together — the doctors and caregivers. A resilient health system cannot rest on fatigued shoulders; valuing both their service and their well-being is the foundation of equitable and sustainable healthcare for rural India.
Recap: